

Overtraining Among Endurance Athletes – Factors and Recommendations for Prevention
by Joseph Giandonato, PhD, MBA, CSCS
NSCA Coach
June 2026
Vol 13, Issue 2
This article discusses overtraining risk factors in endurance athletes and provides strategies for monitoring stress, optimizing performance, and creating effective programming.
INTRODUCTION
In this article, risk factors for overtraining among endurance athletes will be presented and explored. Additionally, strength and conditioning professionals will be provided strategies to monitor training stressors via collection of biomarkers and performance indicators to ascertain health and readiness of the endurance athlete and actionable measures to formulate programming that is effective, efficient, and safe. Overtraining is characterized by an imbalance in training stimuli and recovery, which has been shown to evoke subjective feelings of fatigue and staleness, as well as eventuate decrements in athletic performance (4,9). A prolonged imbalance in training and recovery or a disproportionate amount of or abrupt increase in frequency, intensity, time, or type of activity may elicit overtraining syndrome, a condition characterized by disruptions in autonomic nervous system, neuroendocrine, immunological, and metabolic functioning (9).
Moreover, psychological disturbances, including alterations in mood and increases in anxiety and incident depression may result (9,16). Athletes who engage in training that is too voluminous or frequent face greater musculoskeletal injury risk. In particular, endurance runners face greater injury risk that is attributed to a high volume of ground contacts occurring during the early stance phase of running during which ground reaction forces measure 2 – 3 times bodyweight (3,5). Common overuse injuries among runners include medial tibial stress syndrome (“shin splints”), Achilles tendonitis and tendinopathy, plantar fasciitis and tendinopathy, iliotibial band (IT band) syndrome, tibial stress fractures, patellofemoral pain syndrome, and piriformis syndrome (10,19). Among cyclists, chronic injuries of the lower back, knees, and groin are most prominent, while upper extremity and knee injuries are most common among swimmers, though their incidence and severity are contingent upon years of experience and the type of stroke employed (21,23).
OVERTRAINING RISK FACTORS
A constellation of variables inclusive of lifestyle, health behaviors, training history, and overall health status may contribute to overtraining. An imbalance between training and recovery has been established to precipitate overtraining among athletes (22). Specific to endurance athletes, excessive training load, monotonous training, and increased number of competitions were all found to perpetuate overtraining in addition to increased injury risk (8). Blunted recovery in the form of disrupted sleep, suboptimal nutritional status, and chronic dehydration also can influence overtraining risk (8,17,18). Further, prior illness or exposure to altitude or environmental conditions that the athlete is not accustomed to can contribute to the development of overtraining syndrome (12). Additionally, psychological stress, travel, and the cumulative physiological stress incurred by frequent practices and training can amplify overtraining risk (9). Athletes subjected to a sudden increase in training load without adequate recovery may experience tempered immunological functioning, resulting in an increase in heightened pathogen risk, including upper respiratory tract infections and blunted neuroendocrine functioning characterized by reductions in nocturnal catecholamines, pulsatile luteinizing hormone secretion, ß-endorphin, thyroid stimulating hormone, and growth hormone concentrations (1,9). Myocellular alterations have also been implicated in precipitating overtraining syndrome such as chronic intramuscular glycogen depletion, the accretion and residual deposition of exercise byproducts such as creatine kinase, lactate, oxypurines, and other metabolites, prolonged exercise-induced inflammation, and macrotrauma resulting from prolonged exposure to training stressors with insufficient recovery (6).
IDENTIFYING OVERTRAINING
Overtraining can be attributed to an assemblage of intraindividual characteristics such as lifestyle, health behaviors, training history, and overall health status and may present differently among a wide range of athletes. Responses to training loads are highly variable and strength and conditioning coaches who are responsible for greater numbers of athletes or larger teams may not be able to aptly detect overtraining nor have time to determine its exact cause. In consideration of this, strength and conditioning coaches and those coaching or consulting endurance athletes should maintain adequate training records to enable the quantification of training load. For endurance athletes, measures may include rating of perceived exertion (RPE) and duration in minutes or calculating and subsequently tracking percentages of heart rate reserve, VO₂ reserve, and/or maximal heart rate. Dissemination of instruments, such as a visual analog scale or Likert scale to assess soreness, fatigue, energy, and focus, can provide coaches with valuable and actionable data. If resources are available, isometric grip strength assessments via hand dynamometer, postprandial blood draws, and heart rate variability monitoring may be conducted to ascertain training status and overtraining risk (7,9,14). Additionally, event performance times can be assessed, but decrements observed at this point are ostensibly indicative of overtraining.
PROGRAMMING CONSIDERATIONS
Programming for endurance athletes could be mapped out to include periodized preparation, competitive, and transitional phases. Periodization for endurance athletes should be structured around competitive events or leading up to a competitive season. Preparation of endurance athletes entails three critical phases: a general physical preparedness or aerobic endurance phase, a specific physical preparedness or aerobic endurance plus specific endurance phase, and finally a specific endurance phase that carries into the competitive phase in which training volume is reduced while intensity is maintained (2). The general physical preparedness phase covers the development of aerobic capacity or an “aerobic base” through lower intensity, but higher volume and more frequent training sessions during the early off-season. The subsequent specific physical preparedness phase builds upon intensity, volume, and frequency as the athlete transitions into the competitive season or nears an event. The culminating competitive phase marks the season in which the endurance athlete is competing and is accompanied by a slate of events. It is during this phase that overtraining risk among endurance athletes is highest (11).
Tapering strategies can be employed leading up to an event following a functional overreaching period punctuated by brief reduction in both training volume and intensity, but particularly volume (15). Tapering is aimed at conferring improvements in focus, nutritional status, and musculoskeletal health. A taper of three weeks was found to improve race performance by 3% among highly-trained distance runners owing to attenuated inflammation, increased myosin heavy chain IIa fiber type diameter, peak force, and absolute power (13).
TAPERING
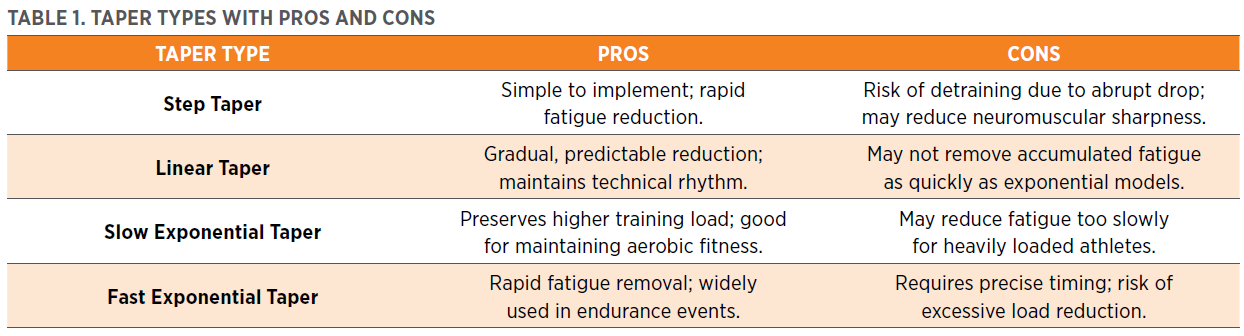
Specific tapering strategies can be employed among endurance athletes to maintain musculoskeletal health, optimize performance, and mitigate overtraining risk. Types of tapering strategies which entail the manipulation of training variables, specifically volume, frequency, and intensity, have been outlined in the research (15,20). The four primary tapering strategies include step tapering, linear tapering, slow exponential tapering, and fast exponential tapering (20).
Step tapering involves a sharp reduction in volume that may encompass reductions of up to 50% of training volume while maintaining intensity. Step tapers are ordinarily implemented 1 – 2 weeks prior to a competition to prioritize health recoverability while enabling the athlete to train at or near race pace. For example, a collegiate cross-country runner logging 50 miles per week will reduce their weekly mileage to 25 miles per week in the weeks leading up to an event. Findings from a meta-analysis involving 14 studies on endurance athletes demonstrated that step tapering significantly improved time-trial performance and time-to-exhaustion performance (20).
Linear tapering entails a reduction in volume that can be implemented weekly or in successive training sessions. Linear tapering can be accompanied by consistent monitoring of performance and recoverability to guide reductions in training variables, specifically volume. Exponential tapering encompasses a reduction in volume at a rate that is proportionate to its current value and is classified as either “slow” or “fast.” A slow exponential taper, for example, would entail reductions of 5% in perpetuity, translating to a reduction of 5% of each successive session. A fast exponential taper is characterized by an aggressive reduction in volume that is substantially greater than a slow exponential taper and is best deployed with precision, especially if in close proximity to an event. Fast exponential tapering differs from step tapering as peaking for competition is prioritized over preserving the health of the athlete. Taper periods spanning three weeks enable a sufficient reduction in volume that can facilitate improvements in performance while upholding health. The selection of a tapering strategy is predicated upon the athlete’s health, training status and level of fitness, and the proximity of the event when the taper is initiated.
Table 1 expands on the four primary taper types for endurance athletes, summarizing the potential pros and cons.
CONCLUSION
In summary, it is imperative that strength and conditioning coaches educate endurance athletes and coaches on the risk factors and dangers associated with overtraining. From the outset, the management of training variables, specifically volume, is critical given the cumulative nature and insidious progression of overtraining and attendant overuse injuries. Some of the time spent building aerobic capacity might be deleterious to the health and performance of the athlete and should be reappropriated to include a complementary resistance training program and supportive recovery modalities. Training programs should entail sensible, and evidence-based approaches that employ periodization and tapering that both consider individual characteristics of the athlete and carefully balance the cardinal programming parameters of frequency, intensity, time, and type to mitigate the risk of overtraining.
This article originally appeared in NSCA Coach, a quarterly publication for NSCA Members that provides valuable takeaways for every level of strength and conditioning coach. You can find scientifically based articles specific to a wide variety of your athletes’ needs with Nutrition, Programming, and Youth columns. Read more articles from NSCA Coach »
REFERENCES
1. Bellinger, P. Functional overreaching in endurance athletes: a necessity or cause for concern? Sports Medicine50(6):1059-1073, 2020.
2. Bompa, TO. Periodization: Theory and Methodology of Training. Champaign, IL: Human Kinetics; 1999.
3. Boullosa, D, Esteve-Lanao, J, Casado, A, Peyré-Tartaruga, LA, Gomes da Rosa, R, and Del Coso, J. Factors affecting training and physical performance in recreational endurance runners. Sports 8(3): 35, 2020.
4. Carrard, J, Rigort, A, Appenzeller-Herzog, C, Colledge, F, Königstein, K, Hinrichs, T, and Schmidt-Trucksäss, A. Diagnosing overtraining syndrome: A scoping review. Sports Health 14(5): 665-673, 2021.
5. Cavanagh, PR, and Lafortune, MA. Ground reaction forces in distance running. Journal of Biomechanics 13(5): 397-406, 1980.
6. Cheng, AJ, Jude, B, and Lanner, JT. Intramuscular mechanisms of overtraining. Redox Biology 35: 101480, 2020.
7. Cronin, J, Lawton, T, Harris, N, Kilding, A, and McMaster, DT. A brief review of handgrip strength and sport performance. Journal of Strength and Conditioning Research 31(11): 3187-3217, 2017.
8. Fiala, O, Hanzlova, M, Borska, L, Fiala, Z, and Holmannova, D. Beyond physical exhaustion: Understanding overtraining syndrome through the lens of molecular mechanisms and clinical manifestation. Sports Medicine and Health Science 7(4): 237-248, 2025.
9. Hoffman, J. Physiological Aspects of Sport Training and Performance. (2nd ed.). Champaign, IL: Human Kinetics; 2014.
10. Konzic, Z, and Sarabon, N. Common running overuse injuries and prevention. Montenegrin Journal of Sports Science and Medicine 6(2): 67-74, 2017.
11. Koutedakis, Y, and Craig Sharp, NC. Seasonal variations of injury and overtraining in elite athletes. Clinical Journal of Sport Medicine 8(1): 18-21, 1998.
12. Kreher, JB, and Schwartz, JB. Overtraining syndrome: A practical guide. Sports Health 4(2): 128-138, 2012.
13. Luden, N, Hayes, E, Galpin, A, Michev, K, Jemiolo, B, Raue, U, et al. Myocellular basis for tapering in competitive distance runners. Journal of Applied Physiology 108(6): 1501-1509, 2010.
14 Lundstrom, CJ, Foreman, NA, and Blitz, G. Practices and applications of heart rate variability monitoring in endurance athletes. International Journal of Sports Medicine 44(1): 9-19, 2023.
15. Mujika, I. Tapering for triathlon competition. Journal of Human Sport and Exercise 6(2): 264-270, 2011.
16. O’Connor, PJ, Morgan, WP, Raglin, JS, Barksdale, CM, and Kalin, NH. Mood state and salivary cortisol levels following overtraining in female swimmers. Psychoneuroendocrinology 14(4): 303-310, 1989.
17. Patel, H, Vanguri, P, Kumar, D, and Levin, D. The impact of inadequate sleep on overtraining syndrome in male and female college athletes 18–22 years old: A literature review. Cureus 16(3): 2024.
18. Puga, TB, Mazumder, RM, Ruan, T, Scigliano, N, Thiel, GE, and Treffer, K. Sleep, nutrition, hydration and rest: the equal importance of external factors outside of training and practice for sports injury prevention. Scientific Journal of Sport and Performance 2(4): 428-438, 2023.
19. Roy, BA. Piriformis syndrome. American College of Sports Medicine Health and Fitness Journal 18(4): 3-4, 2014.
20. Wang, Z, Yong Tai Wang, Gao, W, and Zhong, Y. Effects of tapering on performance in endurance athletes: A systematic review and meta-analysis. PLoS One 18(5): e0282838, 2023.
21. Wanivenhaus, F, Fox, AJS, Chaudhury, S, and Rodeo, SA. Epidemiology of injuries and prevention strategies in competitive swimmers. Sports Health 4(3): 245-251, 2012.
22. Weakley, J, Halson, SL, and Mujika, I. Overtraining syndrome symptoms and diagnosis in athletes: Where is the research? A systematic review. International Journal of Sports Physiology and Performance 17(5): 1-7, 2022.
23. Wilber, CA, Holland, GJ, Madison, RE, and Loy, SF. An epidemiological analysis of overuse injuries. International Journal of Sports Medicine 16(3): 201-206, 1995.
Learn about the benefits of NSCA Membership »
Audience:
Coaches
Coaches
Topics:
Exercise Science Program design Organization and Administration Testing and Evaluation Client Consultation|Assessment Safety Basic Pathophysiology and Science of Health Status or Condition and Disorder or Disease Professional Development
Exercise Science Program design Organization and Administration Testing and Evaluation Client Consultation|Assessment Safety Basic Pathophysiology and Science of Health Status or Condition and Disorder or Disease Professional Development
Keywords:
Physical Preparedness Recovery Physiological Stress Training Volume Periodization Aerobic Training Injury Mitigation Athletic Performance
Physical Preparedness Recovery Physiological Stress Training Volume Periodization Aerobic Training Injury Mitigation Athletic Performance

- Privacy Policy
- Your Privacy Choices

- Terms of Use
- Retraction and Correction Policy
- © 2026 National Strength and Conditioning Association