

Fascial Approach for Enhanced Recovery and Long-Term Survivorship in Breast Cancer Survivors
by Laura Bergmann, PhD, LMT, Bridget Melton, EDD, CSCS, TSAC-F, David Titcomb, PhD, DPT, and Kristen Cochrane-Snyman, PhD, CSCS
Personal Training Quarterly
November 2025
Vol 12, Issue 3
This article discusses how myofascial techniques and prehabilitation can reduce pain, improve mobility, and enhance quality of life for women in breast cancer recovery.
INTRODUCTION
There are approximately 387,850 women diagnosed with invasive breast cancer requiring surgery each year in the United States (2). Nationally, 30% of all new cancer diagnoses are breast cancer, and 54% of those are women under 65 years (2). Women are eager to resume normal daily activities after surgery, but many have long-term pain and movement limitations that inhibit functional movement. The tightening around the surgical site can cause pain in the shoulders, neck, low back, hips, ribs, and even breathing dysfunction (5,10,14). The accumulation of fascial tension is gradual and such effects may take months to get to a level that only causes discomfort when doing daily activities. Gong et al. reported that approximately 28.2% of patients experienced post-mastectomy pain syndrome (PMPS) as early as three months after surgery; it has also been reported that about 60% of women who initially experienced PMPS continued to report symptoms 7 – 9 years post-surgery (14,33). Despite evidence that the combination of myofascial work and exercise is more successful in restoring tissue-based limitations than exercise or tissue work alone, there is no set program for this population before or after surgery (5,10,29). The various types of breast cancer surgery (BCS) are listed in Figure 1.
FASCIAL AND MYOFASCIAL WORK
Myofascial work is commonly known as a technique that focuses on applying fascial holds while moving the tissue at varied pressures and depths (3,7). It refers to a range of manual therapy techniques aimed at assessing and releasing restrictions in the fascial system with the goal of restoring mobility, reducing pain, and improving function. These interventions typically involve sustained pressure and movement through soft tissue to influence the tone, hydration, and alignment of fascia and the underlying musculature. As the fascial system is a continuous three-dimensional network of connective tissue that envelops and interconnects all muscles, bones, and organs, addressing fascial restrictions can have widespread effects throughout the body. The Fascia Nomenclature Committee, developed by the Fascia Research Society, defines the fascial system as “the three-dimensional continuum of soft, collagen-containing, loose and dense fibrous connective tissues that permeate the body... with no discontinuity in its path, with layers of different characteristics and properties overlapping,” (3). This integrated perspective supports the rationale behind myofascial interventions as a means of improving postural integrity and reducing biomechanical stress across multiple regions.
SUPPORT FOR FASCIA FOCUS TECHNIQUES
Self‐myofascial release (SMR) is a popular intervention used by both rehabilitation and fitness professionals to enhance myofascial mobility. Common SMR tools include the foam roller and various types and sizes of roller massagers. Evidence exists that suggests these tools can enhance joint range of motion (ROM) and the recovery process by decreasing the effects of acute muscle soreness, delayed onset muscle soreness (DOMS), and post-exercise muscle performance (4,6,7,11,18,20,23,31). SMR uses an individual’s own bodyweight to apply pressure to the soft tissues with foam rollers and small balls (6,7,31). Direct pressure on the soft tissues combined with micro-movements stretch and compress the tissue, increasing viscosity in adhered areas upon release, decreasing friction between the tissues (28). SMR’s effectiveness in athletic recovery when added to an exercise regimen has been well demonstrated (6,7,12,18,20,23,28,31); with the addition of active movement of a joint when rolling, as opposed to holding the limb still, being the most effective at improving mobility (6). Restoring viscosity to the tissues improves arthrokinematics, and thus may improve function (21).
Benefits of fascia-focused therapy can include (26):
-
- Reduced joint stress (-39%)
- Reduced chronic pains (-73%)
- Reduced trigger point tenderness (-45%)
- Reduced scar size (-24%)
It has been documented that only 8.9% of women who have had BCS meet the current guidelines on aerobic and resistance exercise (19,34). Furthermore, only 40% of oncologists routinely recommend exercise to patients, and only 9% of women who have had BCSs are referred to exercise professionals for continued care (9,32,34). In addition, the combination of fascia work via self-myofascial release and exercise has not been widely utilized despite evidence that decreased mobility due to scarring greatly affects the quality of life (QOL). Therefore, there is a significant need for prehabilitation and post-rehabilitation programs for women who have had BCS.
BEST PRACTICES FOR THE PERSONAL TRAINER
The personal trainer can play an integral role in the journey of their breast cancer clients. This article provides education for personal trainers to help improve mobility and movement patterns to avoid chronic pain, reliance on pain medication, and diminish the risk of future injuries while improving QOL.
WORKING WITH THE HEALTHCARE TEAM
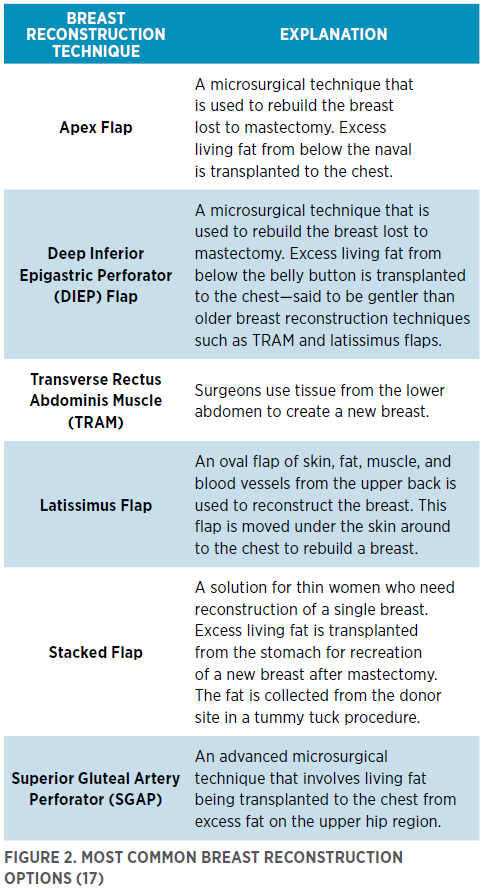
Many reconstruction options involve surgery in other areas, which can affect movement efficiency. It is strongly recommended that a personal trainer becomes familiar with the different types of breast cancer surgeries (Figure 1) and reconstruction techniques (Figure 2) to be able to communicate with the client and their healthcare team adequately. The medical team may include an oncologist, surgeon, reconstruction surgeon, radiologist, physical therapist, lymphedema specialist, massage therapist, and primary care physician, all of whom may want to see notes on sessions completed. The client should get clearance from a physician before beginning any exercise program.
PREHABILITATION
If a client has an opportunity to do prehabilitation before the surgery, they can possibly diminish the forward pull of the upper quadrant (common for most people using phones, computers, and driving) to be able to move in a more neutral alignment (27). A movement analysis must first be done to observe the range of motion and restriction of the upper body including shoulder flexion, extension, internal and external rotation, and abduction. The client should be able to do each movement (with a neutral head position) without harmful kinematic compensation that alters scapula rotation in overhead tasks such as initiating with their upper trapezius/levator (22). While earlier research has raised questions about the relationship between posture, musculoskeletal health, and pain (24), more recent studies have demonstrated clear links between forward head posture (FHP), rounded shoulders like upper crossed syndrome (UCS), and musculoskeletal dysfunction—often affecting an individual’s ability to comfortably perform activities of daily living (13,25). For example, Lotfian et al. found that individuals with FHP exhibit significantly reduced neck extensor endurance and higher levels of pain and disability compared to those with neutral head posture (25). Additionally, Gholami et al. identified a strong association between UCS and upper limb pain, impaired daily function, and decreased quality of life in working women (13). These recent findings underscore the clinical relevance of postural dysfunction, albeit its correlation to pain is not agreed upon. However, a 2024 meta-analysis by Mohammad Pour and colleagues confirmed that targeted therapeutic exercises can effectively improve FHP, reduce thoracic kyphosis, and alleviate related symptoms (27).
Noting the movement compensations will let the personal trainer know what muscles need to move more freely and what has to be strengthened (8). For example, it is common for many people’s shoulders to be anteriorly rotated and tipped with a forward head because of texting, computer work, and driving. Resolving this prior to surgery may be helpful to improve the starting position of the shoulder girdle, as well as get the client comfortable and familiar with the movements. The commonly short areas involved in rounded shoulders and forward head posture include the pectoralis major and minor, anterior scalene, serratus anterior, subscapularis, levator scapulae, sternocleidomastoid, upper trapezius, and posterior cervical spine muscles (15). This disruption of the length-tension relationship leaves the posterior shoulder muscles, such as the middle, lower trapezius, rhomboids, and latissimus dorsi, in a lengthened position, causing a decrease in proper muscle activation. This muscle imbalance alters the scapular and glenohumeral orientation and kinematics, which may contribute to an increased risk of neck, shoulder, nonspecific arm pain, and nerve impingement issues (8,13,16,22,25).
A protracted shoulder has also been implicated in the restricted sliding of the cords of the brachial plexus, thus increasing strain on the various nerves passing through the shoulder region, especially the median nerve (30). Additionally, with this increased kyphosis at the thoracic spine, the anterior longitudinal ligament and the upper abdominal muscles may be shortened, resulting in increased stress throughout the back, and possibly inhibited breathing. In some cases, the brachial plexus in the lateral neck can also be pinched, causing numbness in the fingers.
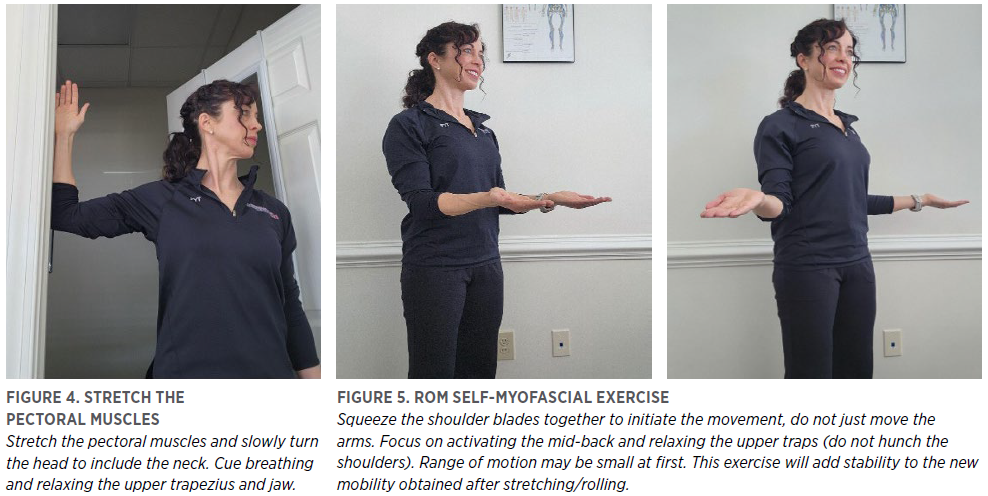
Fascial tissues may lose elasticity and become “sticky” or “dehydrated,” contributing to impaired gliding and functional restriction. Self-myofascial release (e.g., foam rolling) appears to acutely restore tissue slide and range of motion, consistent with a theoretical reduction in viscosity or improved tissue hydration (4,7). A few examples of self-myofascial work are provided in Figures 3, 4, and 5. Placing the client’s hand (gently) or a tennis ball in a door jamb on the area and doing small jostling movements in the desired direction will help hydrate and loosen the area (Figure 3). This should be a small, backward, circular movement for 30 – 60 s, cueing activation of the mid back. Follow with a gentle stretch focusing on slow deep breaths and relaxing the area (Figure 4). Repeat the ROM analysis with coaching to avoid compensation. Repeat until the client can do the movement without compensating, to a pain-free range of motion. It is believed that once the movement patterns are cleaned up, strengthening the previously inhibited or over-stretched muscles can begin. Researchers have suggested that SMR followed by stretching and training the opposing muscle stability can be performed twice weekly for a sustained period (6,8,10). The client will likely do the exercises in their previous compensation patterns as the brain still thinks it has to move that way unless re-patterning is part of the process. A slow tempo is necessary to help the client become more mindful of the new desired movement strategy.
POST SURGERY
LONG-TERM PLAN
During the initial recovery phases after cancer treatment, many patients are referred to physical therapy. However, insurance coverage for rehabilitation is inconsistent, and some treatments may not be covered at all. As a result, patients looking to return or begin exercising may seek the help of a personal trainer for 1 – 7 years post-breast cancer treatment. The muscle imbalances described above lead to alteration in the scapular and glenohumeral orientation, as well as kinematics, thus possibly increasing the risk of developing neck, shoulder, and nonspecific arm pain (13,16,25). These issues are exasperated by the gradual locking down of the upper quadrant as scar tissue forms years after surgery services have been completed. The muscular system and shoulder girdle continue to be pulled forward as the tightening from the scarring increases over the years.

The long-term effects of post-surgical scarring are widespread and often not addressed as part of a post-operative rehabilitation program. Ideally, once the wound has healed and post operative rehabilitation has been completed, a combination of fascia work and exercise should be done and continued as part of a maintenance plan. Post-mastectomy pain syndrome has been seen 1.7 – 7 years after surgery, suggesting that a long-term recovery plan is needed (17). Personal trainers can help women who have had BCS regain mobility and confidence with self-myofascial release and movement retraining long after medical services have ended.
As with the prehabilitation program, a movement assessment is recommended first. Afterward, slow and gentle SMR can be done with a mobility ball around the painful area with micro-movements and breathing by the client. A ball may be used in a door jamb for the pectoralis major and minor and a soft foam roller for the side of the rib cage, teres, and latissimus dorsi. This should be a pain-free experience. Focusing on breathing and small oscillating type movements is key to helping the tissue let go and relax to reestablish sliding and gliding; it should not be painful, which can cause tension and guarding. As mobility and strength improves, the shoulder blade squeezes (Figure 5) can be done with a band to strengthen the weak or elongated muscles as done in prehabilitation sessions. The focus is on improving movement patterns, using a slow tempo and starting with low repetitions and isometric holds (e.g., 5x5 s holds).
INTEGRATION EXAMPLES
After mobility and stability are restored, functional movement can be improved to reintegrate the upper quadrant into daily life movement patterns without compensation. Once all the pieces can work separately, teaching them to all work together without compensating is important. An example would be a squat and band row combined, or a one-arm band push or pull without the upper trap hiking the shoulder up. A squat and overhead press with proper shoulder mechanics and without arching the back is also important as it mimics picking something up and putting it on a shelf.
CONTRAINDICATIONS
As with any SMR protocol, be sure the client is cleared by a physician and does not have a history of or warning signs of blood clots. Although not a contraindication, long after post-operative services have been completed, the client’s skin might still be very sensitive if radiation was also involved, so it is important to choose appropriate tools that are gentle and pain-free. Lymphedema is also an issue that is best handled by a specialist if presented by the client. In most cases, movement is helpful, but caution must be taken when doing any tissue manipulation with those who have a history of lymphedema.
This article originally appeared in Personal Training Quarterly (PTQ)—a quarterly publication for NSCA Members designed specifically for the personal trainer. Discover easy-to-read, research-based articles that take your training knowledge further with Nutrition, Programming, and Personal Business Development columns in each quarterly, electronic issue. Read more articles from PTQ »
REFERENCES
- American Cancer Society. Breast reconstruction options. Updated May 5, 2025. Retrieved July 23, 2025 from https://www. cancer.org/cancer/types/breast-cancer/reconstruction-surgery/breast-reconstruction-options.html.
- American Cancer Society. Key statistics for breast cancer: How common is breast cancer? Retrieved 2025 from https://www.cancer.org/cancer/breast-cancer/about/how-common-is-breast-cancer.html.
- Bordoni, B, and Zanier, E. Skin, fascias, and scars: Symptoms and systemic connections. Journal Multidisciplinary Healthcare 11: 11-24, 2013.
- Bradbury-Squires, DJ, Noftall, JC, Sullivan, KM, Behm, DG, Power, KE, and Button, DC. Roller-massager application to the quadriceps and knee-joint range of motion and neuromuscular efficiency during a lunge. Journal of Athletic Training 50(2): 133-140, 2015.
- Castro-Martín, E, Ortiz-Comino, L, Gallart-Aragón, T, Esteban-Moreno, B, Arroyo-Morales, M, and Galiano-Castillo, N. Myofascial induction effects on neck-shoulder pain in breast cancer survivors: Randomized, single-blind, placebo-controlled crossover design. Archives of Physical Medicine and Rehabilitation 98(5): 832-840, 2017.
- Cheatham, SW, and Stull, KR. Comparison of a foam rolling session with active joint motion and without joint motion: A randomized controlled trial. Journal of Bodyweight and Movement Therapies 22(3): 707-712, 2018.
- Cheatham, SW, Kolber, MJ, Cain, M, and Lee, M. The effects of self-myofascial release using a foam roll or roller massager on joint range of motion, muscle recovery, and performance: A systematic review. International Journal of Sports Physical Therapy 10(6): 827-838, 2015.
- Clark, M, Lucett, S, and Sutton, BG. NASM Essentials of Corrective Exercise Training. 1st ed. Burlington, MA: Jones and Bartlett Learning; 2014.
- Coletta, AM, Marquez, G, Thomas, P, Thoman, W, Bevers, T, Brewster, AM, et al. Clinical factors associated with adherence to aerobic and resistance physical activity guidelines among cancer prevention patients and survivors. PLOS One 4(8): e0220814, 2019.
- De Groef, A, Van Kampen, M, Vervloesem, N, Dieltjens, E, Christiaens, MR, Neven, P, et al. Effect of myofascial techniques for treatment of persistent arm pain after breast cancer treatment: Randomized controlled trial. Clinical Rehabilitation 32(4): 451-461, 2017.
- Dębski, P, Białas, E, and Gnat, R. The parameters of foam rolling, self-myofascial release treatment. Biomedical Human Kinetics 11(1): 36-46, 2019.
- Freiwald, J, Baumgart, C, Kühnemann, M, and Hoppe, MW. Foam-rolling in sport and therapy – Potential benefits and risks. Sports Orthopaedics and Traumatology 32(3): 267-275, 2016.
- Gholami, S, Rastegar, M, Saeedi, H, and Torkaman, A. Prevalence of upper cross syndrome and its association with musculoskeletal pain and functional disability in working women: A cross-sectional study. Journal of Occupational Rehabilitation 34(3): 523-532, 2024.
- Gong, Y, Tan, Q, Qin, Q, and Wei, C. Prevalence of postmastectomy pain syndrome and associated risk factors. Medicine 99(20): e19834, 2020.
- Hardcastle, SJ, Kane, R, Chivers, P, Hince, D, Dean, A, Higgs, D, et al. Knowledge, attitudes, and practice of oncologists and oncology health care providers in promoting physical activity to cancer survivors: An international survey. Supportive Care Cancer 26(11): 3711-3719, 2018.
- Julius, A, Lees, R, Dilley, A, and Lynn, B. Shoulder posture and median nerve sliding. BMC Musculoskeletal Disorder 5(23): 2004.
- Kim, JH, Kim, SH, Kim, HR, Lee, SH, Yoon, SY, Yang, JH, et al. Ultrasonographic evaluation of chronic shoulder pain after breast cancer surgery: Single center, cross-sectional study. Scientific Reports 10(1): 16792, 2020.
- Kiyono, R, Onuma, R, Yasaka, K, Sato, S, Yahata, K, and Nakamura, M. Effects of 5-week foam rolling intervention on range of motion and muscle stiffness. Journal of Strength and Conditioning Research 36(7): 1890-1895, 2022.
- Klein, I, Kalichman, L, Chen, N, and Susmallian, S. Effect of physical activity levels on oncological breast surgery recovery: A prospective cohort study. Scientific Reports 11(1): 2021.
- Konrad, A, Nakamura, M, Tilp, M, Donti, O, and Behm, DG. Foam rolling training effects on range of motion: A systematic review and meta-analysis. Sports Medicine 52(10): 2523-2535, 2022.
- Korucu, TS, Ucurum, SG, Tastaban, E, Ozgun, H, and Kaya, DO. Comparison of shoulder-arm complex pain, function, and scapular dyskinesia in women with and without unilateral lymphedema after breast cancer surgery. Clinical Breast Cancer 21(3): e285-293, 2021.
- Lang, AE, Milosavljevic, S, Dickerson, CR, Kim, SY, and Trask, CM. Scapular kinematics of postmastectomy and postreconstruction breast cancer survivors with and without impingement pain. Annals of Medicine 54(1): 1058-1066, 2022.
- Laudner, K, and Thorson, K. Acute effects of pectoralis minor self-mobilization on shoulder motion and posture: A blinded and randomized placebo-controlled study in asymptomatic individuals. Journal of Sport Rehabilitation 29(4): 420-424, 2019.
- Lederman, E. The fall of the postural-structural-biomechanical model in manual and physical therapies: Exemplified by lower back pain. Journal of Bodyweight Movement Therapy 15(2): 131-138, 2011.
- Lotfian, S, Jafari Fesharaki, M, Shahabbaspour, Z, Akbarzadeh, H, and Moezy, A. The impact of forward head posture on neck muscle endurance and thickness in women with chronic neck pain: A cross-sectional study. BMC Musculoskeletal Disorders 26: 468, 2025.
- Mafu, TS, September, A, and Shamley, D. The potential role of angiogenesis in the development of shoulder pain, shoulder dysfunction, and lymphedema after breast cancer treatment. Cancer Management Research 10: 81-90, 2018.
- Mohammad, Pour, E, Javidan, AN, Salehi, R, et al. The effect of various therapeutic exercises on forward head posture, rounded shoulders, and thoracic kyphosis: A meta-analysis. BMC Musculoskeletal Disorders 25(1): 724, 2024.
- Pearcey, GEP, Bradbury-Squires, DJ, Kawamoto, JE, Drinkwater, EJ, Behm, DG, and Button, DC. Foam rolling for delayed-onset muscle soreness and recovery of dynamic performance measures. Journal of Athletic Training 50(1): 5-13, 2015.
- Serra-Añó, P, Inglés, M, Bou-Catalá, C, Iraola-Lliso, A, and Espí-López, GV. Effectiveness of myofascial release after breast cancer surgery in women undergoing conservative surgery and radiotherapy: A randomized controlled trial. Supportive Care in Cancer 27(7): 2633-2641, 2018.
- Singla, D, and Veqar, Z. Association between forward head, rounded shoulders, and increased thoracic kyphosis: A review of the literature. Journal of Chiropractic Medicine 16(3): 220-229, 2017.
- Sullivan, KM, Silvey, DBJ, Button, DC, and Behm, DG. Rollermassager application to the hamstrings increases sit-and-reach range of motion within five to ten seconds without performance impairments. International Journal of Sports Physical Therapy 8(3): 228-236, 2013.
- Willard, FH., Vleeming, A, Schuenke, MD, Danneels, L, and Schleip, R. The thoracolumbar fascia: Anatomy, function and clinical considerations. Journal of Anatomy 221(6): 507-536, 2012.
- Wiper, A, Jankowski, M, Jabłońska, R, Strychar, J, Zielińska, N, and Sieroń A. Effectiveness of various methods of manual scar therapy. Journal of Clinical Medicine 12(3): 1221, 2023.
- Wirtz, P, and Baumann, FT. Physical activity, exercise and breast cancer – What is the evidence for rehabilitation, aftercare, and survival? A review. Breast Care (Basel) 13(2): 93-101, 2018.
Learn about the benefits of NSCA Membership »

- Privacy Policy
- Your Privacy Choices

- Terms of Use
- Retraction and Correction Policy
- © 2026 National Strength and Conditioning Association