

Rehabilitation to Performance of the Shoulder for the Tactical Athlete
by Alexander Weber, DC, CCSP, CSCS, and Michael Fanning, DC, DACBSP, RMSK, CSCS
TSAC Report
February 2026
Vol 80, Issue 1
This TSAC Report article examines the primary historical and occupational risk factors contributing to shoulder pain in tactical athletes and provides evidence-based rehabilitation strategies.
Shoulder pain is one of the most common upper-extremity musculoskeletal complaints among tactical athletes, a term that encompasses military personnel, law enforcement officers, firefighters, and other first responders (10). Reported incidence of shoulder injuries varies widely, ranging from 8.3% to as high as 43% of all injuries in these populations (10,21). Although shoulder pain is typically multifactorial, chronic symptoms often follow predictable pathological patterns influenced by prior trauma, repetitive occupational demands, participation in overhead sports, congenital or acquired ligamentous laxity, and postural adaptations (1,5,6,7,9,10).
This review examines the primary historical and occupational risk factors contributing to shoulder pain in tactical athletes, outlines relevant patho-anatomy, and provides evidence-based rehabilitation and prehabilitation strategies. By understanding these mechanisms, clinicians and strength and conditioning professionals can implement targeted screening, corrective exercise programming, and load-management strategies to reduce injury risk and restore pain-free function.
HISTORICAL RISK FACTORS
A thorough history remains critical in the evaluation of shoulder pain. Prior participation in overhead sports—such as baseball, swimming, tennis, water polo, or volleyball—significantly increases the likelihood of subsequent shoulder pathology (1,5,6). Previous episodes of glenohumeral dislocation or subluxation markedly elevate recurrence risk and are frequently accompanied by capsular laxity or labral injury (5,7). Cervical spine pathology must also be considered, as referred pain from the cervical region to the scapular or shoulder area is common, often presenting as interscapular or posterior shoulder discomfort (5).
OCCUPATIONAL AND TRAINING-RELATED RISK FACTORS
Overuse injuries are prevalent among tactical athletes because of the repetitive and high-volume nature of both training and operational demands (9,10,21). Large numbers of push-ups performed during physical fitness testing and daily training impose considerable repetitive stress on the shoulder complex, particularly in recruit populations, and should not be overlooked as a contributing factor to pain and injury (21). However, push-ups represent only one component of a broader repetitive-loading profile.
On duty, tactical athletes routinely perform prolonged weapon carrying, heavy load carriage (body armor, hoses, breaching tools, or casualties), overhead tasks during building entry or vehicle extrication, repetitive throwing (flashbangs), and sustained awkward postures (9,10). These activities can lead to subacromial impingement, rotator cuff tendinopathy, labral tears, glenohumeral instability, and biceps pathology (9,10,21).
PATHO-ANATOMY
The shoulder complex consists of the glenohumeral (GH), acromioclavicular (AC), and scapulothoracic (ST) joints. The GH joint, a ball-and-socket articulation between the large humeral head and shallow glenoid fossa, provides the greatest range of motion in the human body but sacrifices inherent bony stability, often compared to a golf ball on a tee (5,9).
This mobility—stability trade-off requires robust static and dynamic stabilizers. Static stabilizers include the glenoid labrum, which deepens the glenoid concavity from roughly 2.5 mm to 5 mm (4,7,9); the joint capsule; the coracohumeral ligament (CHL); and the superior, middle, and inferior glenohumeral ligaments (SGHL, MGHL, IGHL, respectively) (4). Dynamic stabilizers are led by the rotator cuff (supraspinatus, infraspinatus, teres minor, subscapularis), long head of the biceps, and deltoid, with secondary contributions from pectoralis major, latissimus dorsi, and teres major (5,9). Scapulothoracic muscles (serratus anterior, trapezius, rhomboids, pectoralis minor) provide a stable base for the entire complex as they control the position of the scapula (7).
Tactical athletes (or former overhead athletes) utilizing overhead movements can involve repetitive abduction with external rotation stressing the anterior capsule and associated ligaments causing them to stretch over time producing increased external rotation (4,5,14,15). Posterosuperior (SLAP) labral tears can exacerbate humeral head translation by allowing more humeral head movement and further mimic anterior laxity (4,7,15). Conversely, an increase in range of motion with external rotation is typically accompanied by a subsequent loss of internal rotation, termed glenohumeral internal rotation deficit (GIRD; defined as a deficit measuring greater than 20° compared with the non-dominant arm), caused by posteroinferior capsular contracture (4,5,16).
Additionally, the sub-acromial space can become narrowed impinging on tendons and structures that reside within that space. Contracture of the posterior band of the IGHL shifts the humeral head posterosuperiorly during abduction with external rotation, altering the center of rotation for the humeral head in relation to the glenoid (4,16). These kinematic changes, combined with scapular dyskinesis (abnormal positioning of the scapula due to altered shoulder mechanics and lack of stabilizing muscular control), narrow the subacromial space and increase compression of the supraspinatus tendon and biceps tendon, commonly resulting in posterosuperior rotator cuff tears and tendinopathy (4,7,13).
CHRONIC SHOULDER PAIN
Common chronic shoulder injuries include subacromial impingement, rotator cuff tendinopathy, glenoid labral tears (including SLAP lesions), and shoulder instability (4,5). A history of repetitive overhead activity, whether from youth sports such as baseball or from occupational demands, significantly influences current shoulder pain and must be considered when designing exercise programs. Even if an individual has not thrown overhead for decades, prior exposure can produce lasting adaptations collectively known as “thrower’s shoulder” (4,5,15).
Thrower’s shoulder arises from repetitive overhead motion and typically produces specific biomechanical faults (4,5). A hallmark adaptation is posterior glenohumeral joint capsule contracture, which posteriorly shifts the humeral head’s center of rotation. This alteration may also manifest as excessive glenohumeral external rotation coupled with restricted internal rotation, a condition termed glenohumeral internal rotation deficit (GIRD). GIRD has two primary consequences: (1) increased shear forces at the superior labrum, elevating risk of superior labrum anterior-to-posterior (SLAP) tears at the biceps anchor, and (2) concomitant anterior capsule stretching, which promotes anterior glenohumeral instability (4,5,15). Secondary subacromial impingement and rotator cuff overload often follow as the humeral head migrates superoposteriorly during throwing or overhead activity (4,5,11).
Finally, chronic anterior capsule laxity—whether from prior dislocation or repetitive microtrauma—can markedly impair progression of horizontal pressing exercises (4,5,25). During the transition from eccentric to concentric phases of the bench press or push-up, excessive anterior humeral head translation may occur, resulting in painful subluxation or apprehension (4,5,20,25).
ASSESSMENT
REHAB TO PERFORMANCE TEAM
When working with this population, it is highly recommended to have a team of specialists to help return the tactical athlete to duty. The tactical athlete should be seen by a Doctor of Physical Therapy (DPT), Orthopedic Surgeon, or Sports Medicine Chiropractor for clinical pathology prior to beginning a program. While the strength and conditioning specialist may sometimes be the point of access to care tactical athlete, if the tactical athlete has the complaints, they should be assessed by a healthcare provider:
-
- Shoulder pain at night regardless of sleeping position,
- Painful popping and clicking in the shoulder,
- Recurring shoulder dislocations,
- Progressive weakness or recurring numbness and tingling in the arm or hand,
- Failure of conservative care,
- Loss of range of motion or visible atrophy (muscle loss),
- Inability to perform activities of daily living,
Part of the return to performance model should include a clinical examination and diagnosis. A specialist can help determine, in the clinical setting, if the tactical athlete is a good candidate for rehabilitation or if further work-up is necessary. Dynamic orthopedic shoulder examinations are critical in the decision-making process. Though not limited to, an often-used cluster of examinations for shoulder instability are the anterior apprehension test, followed by relocation test then the reverse relocation test (7). This clinical examination should take place prior to any fitness or movement assessment occurs. Lastly, a determination of congenital ligament laxity or suspicion of connective tissue disorder is important.
a. Congenital Ligament Laxity
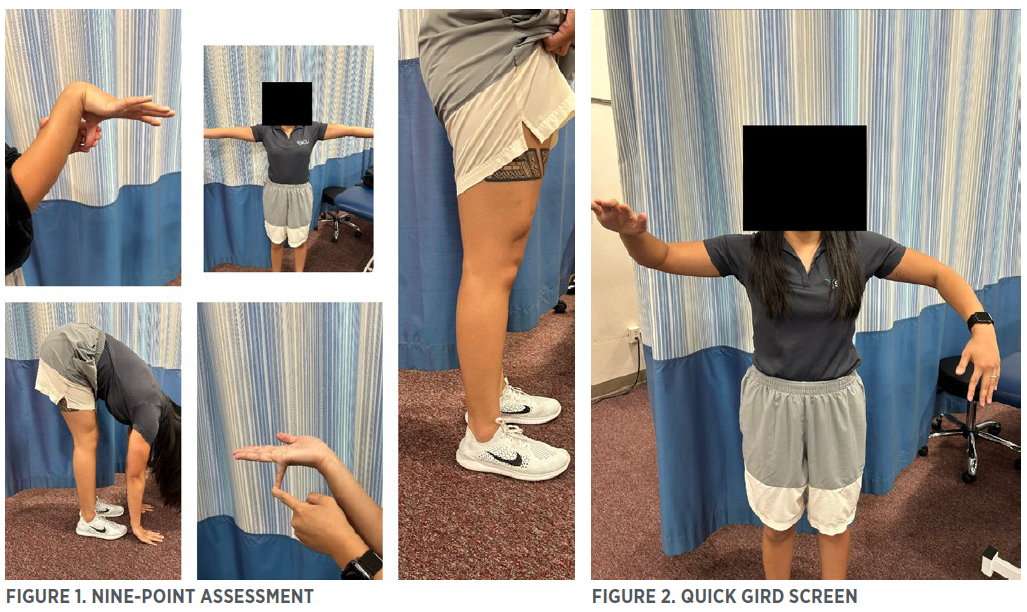
A nine-point assessment should be performed on the tactical athlete to see if congenital joint hypermobility is present. However, this is not diagnostic and can be a screen for the strength and conditioning coach (Figure 1):
-
- Left and right 5th digit passive dorsiflexion beyond 90°
- Left and right thumb passive dorsiflexion to the flexor aspect of the forearm.
- Left and right elbow hyperextends beyond 10°
- Left and right knee hyperextends beyond 10°
- Forward flexion of trunk with knees full extended.
Each joint assessed is one point, for a total possibility of nine points. A score above six indicates global hypermobility (but not necessarily a connective tissue disorder such as Ehlers-Danlos Syndrome (4,5). If an athlete has six of these points, with chronic shoulder problems or difficulty with horizontal presses, for example, the presence of atraumatic multi-directional, rehab as treatment, instability (AMBRI) should be considered.
b. Glenohumeral Internal Rotation Deficit (GIRD)
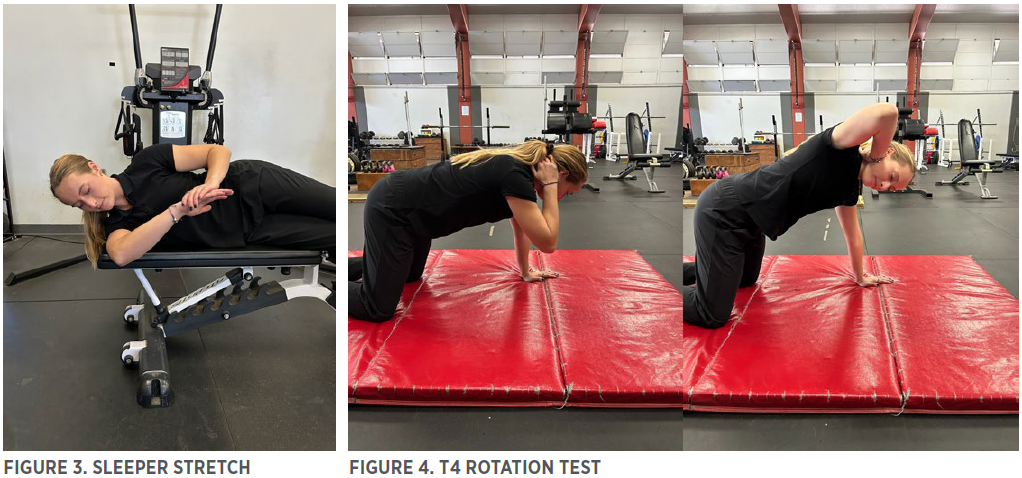
Tactical athletes with GIRD can be asymptomatic. GIRD is an adaptive process in which the dominant shoulder experiences a loss of internal rotation (IR) (4,5,23). Most commonly defined by a loss of >20° of IR compared to the opposite shoulder (4,23). The typical cause of GIRD is posterior glenohumeral ligament (capsule) contracture, as previously discussed. GIRD is often associated with several related diagnosis including subacromial impingement, articular side rotator cuff tears, and glenoid labrum tears (4,5).
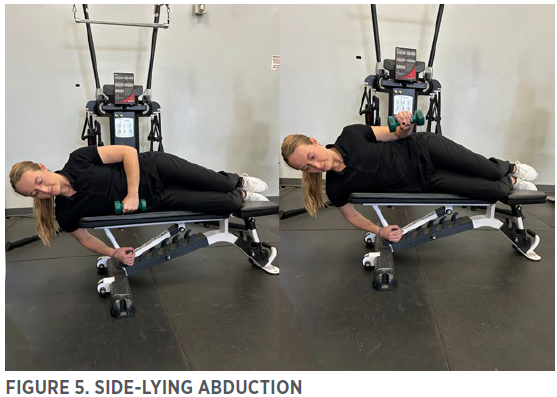
Figure 2 demonstrates a quick screen to see if GIRD is present. This tactical athlete is suspected of having GIRD on his right side. There is a more precise way to measure GIRD, but this requires a partner and a goniometer. If an asymmetry is seen here, the remedy is often “the sleeper stretch” (Figure 3). Try performing this stretch before any pressing workout or overhead activity (swimming included), start with 3 sets of 10 second hold on the affected side.
c. Thoracic spine motion
Persistent shoulder pain should prompt consideration of thoracic spine immobility as a contributing factor. Restricted thoracic extension is frequently associated with shoulder pain and reduced active range of motion (2,8).
Assessing thoracic spine mobility is generally more challenging than assessing cervical or lumbar motion because the thoracic region is inherently less mobile. Several reliable methods exist:
-
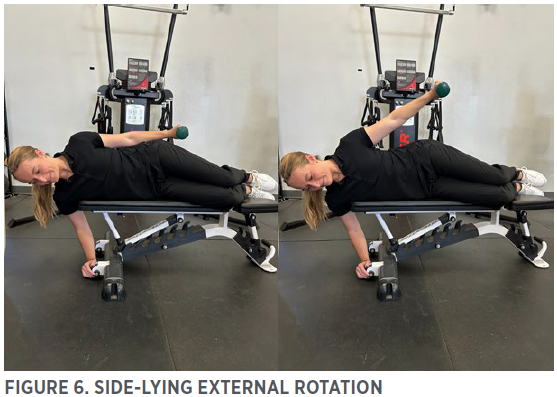
- Thoracic rotation can be evaluated using the “T4 rotation” test (Figure 4).
- Thoracic flexion and extension are best assessed in quadruped or seated positions.
In each case, the patient should move slowly into end-range, hold for 2 – 3 seconds, and stop if pain is provoked. The goal is to identify true mechanical restriction rather than pain-limited motion.
Improved thoracic mobility positively influences scapulothoracic rhythm and overall shoulder range of motion. Notably, one randomized study demonstrated that a thoracic mobility program significantly reduced pain and improved function in patients with chronic rotator cuff tendinopathy (8,20). Although alterations in scapular motion (scapular dyskinesis) are often discussed in this context, the topic remains controversial and is beyond the scope of this article.
REHABILITATION TO PERFORMANCE START POINT
a. Rotator Cuff Exercises
The rotator cuff provides dynamic glenohumeral stability and must remain a cornerstone of both rehabilitation and long-term shoulder health programming for tactical athletes. Imbalances—particularly weakness of the supraspinatus, infraspinatus, and teres minor relative to the stronger internal rotators (subscapularis, pectoralis major, latissimus dorsi)—are common in this population and may contribute to impingement, superior humeral head migration, and secondary labral overload (5,11,18).
High-priority, low-load rotator cuff exercises should be performed 3 – 5 times per week and precede all pressing or pulling sessions. The following three side-lying exercises are safe, effective, and easily progressed (11):
-
- Side-lying Abduction to 45° Primary target: supraspinatus. Maintains humeral head depression during early abduction and counters deltoid-driven superior translation (Figure 5).
- Side-lying External Rotation (arm at side, 0° abduction) Primary target: infraspinatus and teres minor. Directly addresses the external-rotation weakness that exacerbates GIRD, anterior capsule stress, and impingement (Figure 6).
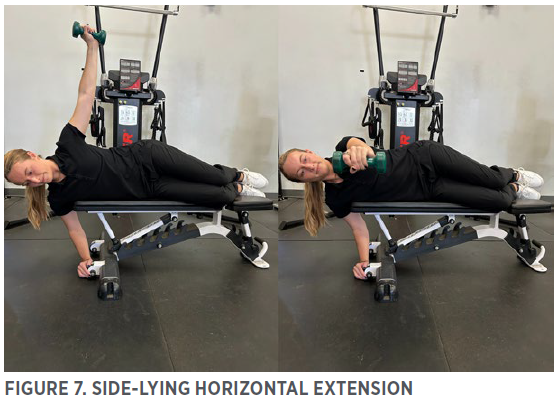
- Side-lying Horizontal Extension (“T” movement, arm in line with torso) Primary target: posterior cuff and lower trapezius/scapular retractors. Reinforces scapular posterior tilt and humeral head centering (Figure 7).
These exercises are non-fatiguing at the prescribed loads yet produce rapid improvements in cuff endurance and glenohumeral force-couple efficiency—essential prerequisites before advancing to compound pressing, pulling, or overhead movements in tactical athletes with chronic shoulder pain (11,18). The following represents prescription guidelines across phases of possible rehabilitation and continued performance-related training (11):
-
- Rehabilitation phase (active pain or recent injury): 1 – 5 lb dumbbell, 3 – 4 sets of 12 – 20 slow, controlled repetitions.
- Prehabilitation/maintenance phase: 5 – 15 lb dumbbell, 3 sets of 10 – 15 repetitions with 2 – 3 s eccentric focus.
- Perform daily or before every upper-body session; fatigue should be localized to the cuff, not the deltoid or neck.
b. Horizontal and Vertical Presses
A fundamental movement pattern in upper body strength training is pressing. The press can be performed horizontally (example: bench press) or vertically (example: an overhead press). Regardless of the type of press, if a shoulder is unstable the tactical athlete may experience pain and potential injury. Modifications can be made to pressing movements to modify the exercise to make it more beneficial and reduce risk of further aggravation to the tactical athlete with an unstable shoulder.
With the vertical press, a more unstable load being pressed overhead may result in greater activation of the shoulder stabilizing musculature (6). This means an overhead press exercise like a machine press is going to require the least amount of stabilization and will make it easier for the humeral head to stay centered in the glenoid socket as compared to a barbell, kettlebell, or dumbbell press. For a tactical athlete with shoulder instability, starting with a machine press may be preferential for pain tolerance and re-establishing baseline strength. Overtime as they become stronger overhead and with concurrent strengthening of the shoulder stabilizing muscles they should be progressed if it can be tolerated. The barbell press should be considered the first progression from a machine press as the dumbbell or kettlebell will require the greatest amount of stabilization to keep the humeral head centered in the glenoid as it is a single arm movement (6).
Research has suggested that using a wider grip with bench pressing increases the compression and shear forces within the glenohumeral joint while horizontal pressing (19). Therefore, if the tactical athlete has an unstable shoulder, they should be able to bench press with less pain and decrease further injury risk by using a narrower grip. Specifically a grip width between 1 and 1.5 bi-acromial widths has been suggested as the most advantageous to minimize compression and shear forces within the GH joint (19). To measure the bi-acromial width of a tactical athlete, a measurement is taken from one acromion process to the other. Noteboom et al. (19) also found that maintaining a retracted scapula can also decrease the GH compressive and shearing forces experienced during a bench press. By using a narrower grip and keeping the scapula retracted during the bench press, the tactical athlete with an unstable shoulder should be able to minimize the amount of compression and shear forces that the GH joint goes through during the movement (19). This will hopefully minimize the need for reliance on the stabilizing structures of the shoulder as the humeral head stays centered in the glenoid (19,24).
c. Horizontal and Vertical Pulls
Prior to integrating any horizontal or vertical pulls, it is important to ensure there is appropriate rotator cuff strength and stability. Both horizontal and vertical pulling exercises can be initiated once the tactical athlete has progressed in the rudimentary side-lying rotator cuff exercises discussed above. Without adequate rotator cuff strength, there is increased stress placed on the glenohumeral joint itself (2). Vertical pulling exercises, such as the latissimus dorsi “pull-down” and the horizontal pulling exercises, such as the seal row or bent over row can be used in both rehabilitation settings and ongoing performance training for those with chronic shoulder pain. These exercises involve the shoulder as they target, but not exclusively, the teres major and latissimus dorsi, both of which are dynamic shoulder stabilizers.
The latissimus dorsi exercise should be performed in front of the neck while avoiding full extension of arms to avoid excessive shearing forces at the glenoid (2). Additionally, the intent of avoiding the “pull-down” behind the neck is to avoid excessive stress at the anterior glenohumeral ligament complex (2). Neutral, supination and/or pronation grip can be used with a narrower spacing. Aggressive, rapid movements should be avoided with a focus of the eccentric portion of the exercise to avoid the previously discussed shearing at the glenoid (2). Furthermore, the bent-over row is a great exercise selection for tactical athletes with instability as the exercise limits stress placed on the anterior glenohumeral capsule. Optimizing this lift should include a neutral grip, with arm abduction less than 30° (2).
d. Lateral Raise
The lateral deltoid raise is a popular exercise to strengthen the deltoid and the entire shoulder complex. The biggest issue with the lateral deltoid raise is that when the shoulders are abducted with internal rotation, impingement of the supraspinatus can occur between the humeral head and the acromion process (4,11). If a tactical athlete has an unstable shoulder, this impingement can become more pronounced due to the superior migration of the humeral head that has been observed with unstable shoulders. For example, Kolber et al. (16) found that maximum shoulder impingement occurred above 90° of abduction. Therefore, the first strategy for tactical athletes training with an unstable shoulder that want to perform the exercise should stop the range of motion below 90° of abduction. Additionally, it was found that the strength of the rotator cuff had an inverse relationship with symptoms of shoulder impingement. This relationship shows that a stronger rotator cuff can be useful to minimize the superior translation of the humeral head ultimately decreasing impingement. Therefore, tactical athletes that still experience impingement symptoms while keeping the range of motion below 90° of abduction could benefit from strengthening of the rotator cuff (16).
e. Squat
Commonly used bar placements while back squatting are the low- or high-bar position. In a low-bar back squat, the bar is placed along the posterior deltoid and the middle trapezius. This position allows the lifter to utilize a more horizontal torso position and target the hip extensors (glutes and hamstring) more effectively than a high bar squat where the quadriceps are more effectively targeted (22). This low-bar position can cause anterior dislocations and impingement in the shoulder because of the external rotation required at the shoulder and the load being placed directly on the shoulder (6). In the tactical athlete that has instability in the shoulder, this position is even more likely to cause pain and injury. For this reason, in tactical athletes with an unstable shoulder itis recommended to utilize a high bar position or even a safety squat bar. With the high bar position, the bar is placed on top of the upper trapezius and requires a more vertical torso angle. Using this position the tactical athlete can decrease the amount of force that is exerted into the shoulder and will likely be able to squat with less shoulder pain and chance of injury. Another strategy to even further decrease the force into the shoulder is to utilize a safety squat bar. A safety squat bar is a specialized cambered shaped barbell with shoulder support that removes the requirement for external rotation at the shoulder altogether. By completely removing external rotation at the shoulder the tactical athlete with an unstable shoulder will have the least risk and compromise to the shoulder.
CONCLUSION
Shoulder pain in tactical athletes is highly prevalent, often chronic, and multifactorial. Repetitive occupational demands (load carriage, weapon handling, overhead tasks, and high-volume push-ups), combined with historical risk factors such as prior overhead sports participation, traumatic dislocations, GIRD, and congenital or acquired capsular laxity, create predictable patterns of subacromial impingement, rotator cuff tendinopathy, labral pathology, and glenohumeral instability.
Effective management requires a systematic, collaborative approach. Early clinical screening by qualified providers (physical therapists, sports chiropractors, or orthopedic specialists) is essential to rule out red flags and guide decision-making. Strength and conditioning professionals play a critical role in subsequent prehabilitation and rehabilitation by 1) identifying range-of-motion deficits (especially GIRD, thoracic mobility restrictions, and hypermobility), 2) prioritizing rotator cuff and scapular stabilizer strength, and 3) progressively modifying foundational movements (horizontal and vertical pressing and pulling, squatting, and lateral raises—to minimize excessive glenohumeral translation, shear, and impingement while restoring load tolerance.
When historical, occupational, and biomechanical risk factors are systematically addressed through targeted assessment and evidence-informed exercise selection, most tactical athletes with chronic shoulder pain can return to full operational duty with reduced pain, improved resilience, and lower risk of recurrence. A proactive, team-based model that bridges clinic and gym ultimately protects both the individual operator and the mission.
This article originally appeared in TSAC Report, the NSCA’s quarterly, online-only publication geared toward the training of tactical athletes, operators, and facilitators. It provides research-based articles, performance drills, and conditioning techniques for operational, tactical athletes. The TSAC Report is only available for NSCA Members. Read more articles from TSAC Report
REFERENCES
- Barrett, E, O’Keeffe, M, O’Sullivan, K, Lewis, J, and McCreesh, K. Is Thoracic Spine Posture Associated with Shoulder Pain, Range of Motion and Function? A Systematic Review. Manual Therapy 26: 38–46, 2016.
- Bleacher, J, and Ellenbecker, TS. Modification of traditional exercises for shoulder rehabilitation and a return-to-lifting program. In: Shoulder Rehabilitation: Non-Operative Treatment 107, 2006.
- Bokshan, SL, DePasse, JM, Eltorai, AEM, Paxton, ES, Green, A, and Daniels, AH. An evidence-based approach to differentiating the cause of shoulder and cervical spine pain. The American Journal of Medicine 129(9): 913–918, 2016.
- Burkhart, SS, Morgan, CD, and Kibler, WB. The disabled throwing shoulder: Spectrum of pathology Part I: pathoanatomy and biomechanics. Arthroscopy 19(4): 404-420, 2003.
- Burkhart, SS, Morgan, CD, and Kibler, WB. The disabled throwing shoulder: Spectrum of pathology Part III: The SICK scapula, scapular dyskinesis, the kinetic chain, and rehabilitation. Arthroscopy 19(6): 641-661, 2003.
- Coratella, G, Tornatore, G, Longo, S, Esposito, F, and Cè, E. Front vs back and barbell vs machine overhead press: An electromyographic analysis and implications for resistance training. Frontiers in Physiology 13: 825880, 2022.
- Cutts, S, Prempeh, M, and Drew, S. Anterior shoulder dislocation. The Annals of The Royal College of Surgeons of England 91(1): 2–7, 2009.
- DeFroda, SF, Goyal, D, Patel, N, Gupta, N, and Mulcahey, MK. Shoulder instability in the overhead athlete. Current Sports Medicine Reports 17(9): 308-314, 2018.
- Gill, TK, Shanahan, EM, Tucker, GR, Buchbinder, R, and Hill, CL. Shoulder range of movement in the general population: age and gender stratified normative data using a community-based cohort. BMC Musculoskeletal Disorders 21(1): 676, 2020.
- Holloway-Beth, A, Forst, L, Freels, S, Brandt-Rauf, S, and Friedman, L. Occupational injury surveillance among law enforcement officers using workers’ compensation data, Illinois 1980 to 2008. Journal of Occupational and Environmental Medicine 58(6): 594–600, 2016.
- Horrigan, J, and Robinson, J. Seven-Minute Rotator Cuff Solution. Health FORLIFE; 1991.
- Ingram, S. Taking a comprehensive health history: learning through practice and reflection. British Journal of Nursing 26(18): 1033–1037, 2017.
- Howe, L, and Waldron, M. Measuring range of motion: A strength and conditioning coach’s guide to assessing mobility. Strength and Conditioning Journal 7–17, 2019.
- Keller, RA, De Giacomo, AF, Neumann, JA, Limpisvasti, O, and Tibone, JE. Glenohumeral internal rotation deficit and risk of upper extremity injury in overhead athletes: A meta-analysis and systematic review. Sports Health 10(2): 125-132, 2018.
- Kinsella, SD, Thomas, SJ, Huffman, GR, and Kelly, JD. The thrower’s shoulder. Orthopedic Clinics of North America 45(3): 387–401, 2014.
- Kolber, M, Cheatham, S, Salamh, P, and Hanney, W. Characteristics of shoulder impingement in the recreational weight-training population. Journal of Strength and Conditioning Research 28(4): 1081-1089, 2014.
- Lin, DJ, Wong, TT, and Kazam, JK. Shoulder injuries in the overhead-throwing athlete: epidemiology, mechanisms of injury, and imaging findings. Radiology 286(2): 370-387, 2018.
- McCausland, C, Sawyer, E, Eovaldi, BJ, and Varacallo, M. Anatomy, Shoulder and Upper Limb, Shoulder Muscles. Treasure Island, FL: StatPearls Publishing; 2025.
- Noteboom, L, Belli, I, Hoozemans, MJM, Seth, A, Veeger, HEJ, and Van Der Helm, FCT. Effects of bench press technique variations on musculoskeletal shoulder loads and potential injury risk. Frontiers in Physiology 15: 1393235, 2024.
- Omoumi, P, Teixeira, P, Lecouvet, F, and Chung, CB. Glenohumeral joint instability. Journal of Magnetic Resonance Imaging 33(1): 2-16, 2011.
- Owens, BD, Duffey, ML, Nelson, BJ, DeBerardino, TM, Taylor, DC, and Mountcastle, SB. The incidence and characteristics of shoulder instability at the United States military academy. The American Journal of Sports Medicine 35(7): 1168-1173, 2017.
- Rash, J. The shoulder and heavy squatting. Strength and Conditioning Journal 22(4): 49, 2000.
- Rose, MB, and Noonan, T. Glenohumeral Internal rotation deficit in throwing athletes: Current perspectives. Open Access Journal of Sports Medicine Volume 9: 69–78, 2018.
- Tillaar, R, and Ettema, G. A comparison of muscle activity in concentric and counter movement maximum bench press. Journal of Human Kinetics 38: 63–71, 2013.
- Wilk, KE, Arrigo, CA, and Andrews, JR. Current concepts: the stabilizing structures of the glenohumeral joint. Journal of Orthopaedic and Sports Physical Therapy 25(6): 364-379, 1997.
Learn about the benefits of NSCA Membership »
Audience:
TSAC Facilitators
TSAC Facilitators
Topics:
Exercise Science Exercise Technique Organization and Administration Testing and Evaluation Client Consultation|Assessment Safety Basic Pathophysiology and Science of Health Status or Condition and Disorder or Disease Professional Development
Exercise Science Exercise Technique Organization and Administration Testing and Evaluation Client Consultation|Assessment Safety Basic Pathophysiology and Science of Health Status or Condition and Disorder or Disease Professional Development
Keywords:
Rehabilitation Shoulder Exercises First Responders Injury Prevention Exercise Research LTAD Occupational Fitness Pathology
Rehabilitation Shoulder Exercises First Responders Injury Prevention Exercise Research LTAD Occupational Fitness Pathology

- Privacy Policy
- Your Privacy Choices

- Terms of Use
- Retraction and Correction Policy
- © 2026 National Strength and Conditioning Association